
The Pandemic's Wrongest Man Is Spreading Misinformation About Vaccine Side Effects in Teens
Have you been hearing some worrisome claims about the vaccines and CDC data and something about heart inflammation? You've come to the right fact check.
Claims appear here,1 here,2 and here.3 These articles reference the same source material, a CDC presentation given on June 23, 2021.4 The slides outline what is known about the risk of myocarditis to 12-15-year-olds receiving the mRNA vaccine.
The claims in this fact check come from an article by Alex Berenson, a journalist known for making claims that conflicted with experts throughout the Covid-19 pandemic.5
No one is right all the time, but an article detailing false and misleading claims from this author published in April 2021 in The Atlantic with the title: The Pandemic’s Wrongest Man.6

Given the author’s lack of relevant expertise, Hoaxlines cannot exclude misinterpretation or inexperience as the driving force behind the false or misleading information. We, therefore, classify misleading or false claims from this author as misinformation.7

To date, the article containing the claims assessed in this fact check has been cited in other vaccine misinformation articles with titles like
Bombshell: ‘Vaccine’ More Dangerous Than Covid-19
CDC Data Highlights COVID Vaccination is More Dangerous than COVID Infection for Young Adults
Vaccine damage to children more severe than COVID
Misinformation, like the coronavirus, spreads rapidly. False claims spread much faster than the facts,8 so let’s take a look at the misinformation that appears to be spreading at the speed of light.
Claim One
At the meeting, CDC scientists presented horrendous data. It showed that even without accounting for underreporting, a second dose of the Pfizer and Moderna vaccines could increase the risk of problems up to 200-fold in young men.
Assessment: It’s unclear how Berenson defines “problems.” If that includes soreness in the arm or mild fever, this differs significantly from if the 200-fold increase is for heart inflammation alone. Without a definition, it’s not possible to assess the claim.
There also appears to be some discrepancy where the rate of myocarditis used in the author’s claims includes those 29 years or younger, while the Covid infection outcomes for comparison come from a different age group.
That’s not necessarily problematic if considered in the analysis, but I did not see any consideration of this detail.
Claim Two
In all of 2019, the CDC’s voluntary vaccine side effect reporting system received about 48,000 reports for ALL vaccines. So far in 2021, it has received at least seven times that many for Covid vaccines alone.
Short Answer: Exponentially increased reporting is expected because of the unprecedented rate of vaccination and people being required to report anything even possibly related.
Even without that detail, the data are not alarming because reporting currently requires providers to submit deaths and serious illnesses even if they know it isn’t related to the vaccine if it happens within a specified time after the vaccination.9
Long Answer: The increase is unsurprising with a new vaccine out, anxiety about vaccine side effects, and unprecedented rates of vaccination. Typically vaccines are administered to infants and children and then periodically as an adult, with the exception of the flu vaccine.10 That alone could reasonably explain the increase, but the statement is further troubling because it is based on VAERS.
Using VAERS presents two problems:
VAERS doesn’t show whether the reported case is caused by a vaccine11 and
The 12-to 15-year-olds were monitored with V-safe, a completely separate monitoring system.12
That they were monitored by V-Safe was clearly disclosed in the presentation, which also included information about VAERS.


VAERS is a fantastic screening tool, and like all screening tools and as the presentation makes abundantly clear, it has a high rate of false positives. This means many entries in the system are not related to the vaccine.
The database currently includes 27 deaths attributed to suicide.13 It is safe to say that those were not related to the vaccine. There are many other deaths and instances of serious illness that are not related to the vaccine. The reality may be that the majority of entries are unrelated.

How did they end up in the database then, if it’s so clear the deaths weren’t related?
To ensure that misjudgment didn’t cause us to miss a very rare side effect where a single case may determine whether or not we detect it, all deaths and serious health events following the Covid-19 vaccine, related or unrelated, had to be reported via VAERS.
The directions for data entry explicitly mandate providers enter life-threatening illness or deaths even if the vaccine is not the cause, within a certain time frame after the vaccine.14 This can be seen on the website as well.
Catching a lot of false positives is not abnormal for screening tools designed to have a high sensitivity because ending up with a lot of false positives also means not missing true positives.15
Determining whether a case is a true or false positive is not something that can be done without access to patient records and significant experience, generally. There are exceptions like cases of suicide or deaths from trauma like car accidents, but generally, it’s not possible. We should also consider that with millions and millions of doses given throughout the world that people will die and it won’t necessarily relate to the vaccine.
It could—which is why we’re reporting and investigating deaths following vaccination—but dying after vaccination is not itself proof. To assume the vaccine caused the death with no other evidence is like saying everyone who died drank water the week before, so the water is killing them. It probably wasn’t the water.
Someone might die after infection from Covid, for example, but whether a death certificate says that Covid caused the death depends on what went wrong in a person’s body. If they drowned, Covid wasn’t the cause. If they developed pneumonia or had a stroke or heart attack related to the blood clotting abnormalities the virus can cause, then yes, the virus would be recorded as a cause of death. You need access to medical records to assess the death.
Claim Three
In fact, the CDC’s own data shows that for every 100,000 vaccines given to young people, more than 25,000 will have temporary side effects that prevent them from “normal activities,” 700 will require medical care and 200 will be hospitalized.
Answer: Another way of saying this is that 1 in 4 people who get the vaccination have a fever or headache. Typically numbers are reduced because smaller numbers make it easier for us to understand our risk. Large numbers make it harder to meaningfully understand our risk and may make a bad outcome appear more common than it is.
Looking at hospitalizations, there are a few factors to consider. The data show 3142 hospitalizations in the 0-17 age bracket. The author references data that conflicts with the overall conclusion of the CDC. This likely reflects that they did not merely consider one data set, but multiple studies. There were earlier hospitalization rate studies, the presentation cites Covid Net, and there are other sources of data.

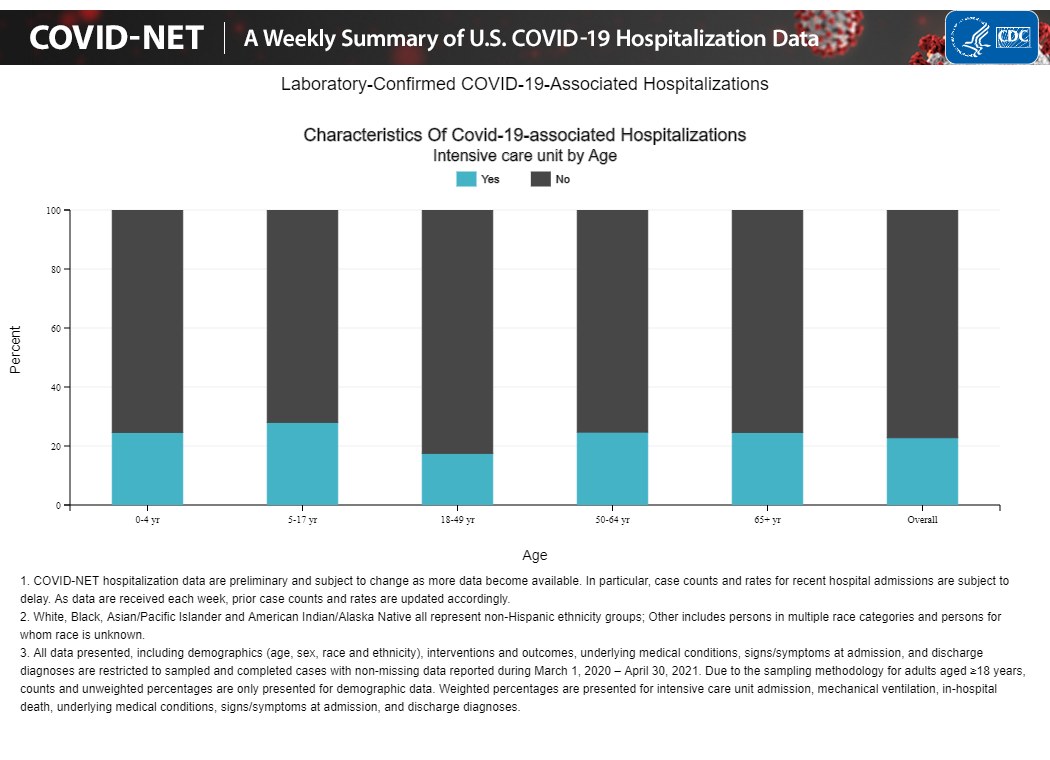
While children are less likely to require hospitalization, we can see that they have some of the highest rates of ICU care when they are admitted, even higher than the 65+ age bracket.16 Kids who are admitted for Covid-19 often need critical care and the consequences of that can last a lifetime. Mechanical ventilation damages the lungs, as an example.
As of June 17, there have been 4,024,335 total child COVID-19 cases reported.17
Looking at the hospitalizations (3,142 in the under 18 bracket), this makes up 0.08% of the reported cases. There have been 314 deaths from Covid infection in under age 18.

Let’s convert the numbers to per 100,000 since the original author used that.
78 hospitalizations per 100,000 infection cases among those under 18 years.

The rate of death from infection is 7.8 per 100,000 recorded cases among those under 18 years of age. This uses the most recent case counts from the American Academy of Pediatrics18 and CDC death data.
This number is almost certainly somewhat inflated because we find more severe cases while mild cases go undetected. Some states had relatively high percent positive testing among kids, suggesting that we may have been missing a considerable number of cases. We should keep that in mind when considering the data but that does not mean it’s completely useless.
To play devil’s advocate, let us assume that every child in the US has already had Covid, which is obviously not the case, the rate of death from infection as of right now would be 0.43 deaths from infection if the entire child population in the US had already been infected per 100,000 (314 deaths/73,000,000 under 18).19
About 25 to 26 deaths in the 12 to 15-year-old age range from the vaccine would make it roughly equal in lethality to infection (around 6,000,000 doses were given to the 12 to 15-year-old group in May and June).20

Remember, there would have to be 25 to 26 vaccine-related deaths among 12 to 15-year-olds right now for the vaccine to be equally deadly, assuming the absolute lowest possible number of deaths from the infection right now because we calculated under the assumption all children had been infected.
There is at most one possible death, but that’s not certain. The cause of death has not been released—-meaning it could be a car accident. We just don’t know.
In the 29 years-and-under mRNA-vaccine group, there were 2 people who required intensive care.21 Compare that to the far higher rate of ICU care among infected children.
Children have not all been infected. The American Academy of Pediatrics estimated the all-time rate of infection among those under 18 to be 5346.8 per 100,000.
What that means is the vaccine is significantly safer. There are a lot more children who could become infected and that will further improve the benefit profile as infection accumulates more deaths and the vaccine do not.
Problems of the Heart
The rate of myocarditis from the vaccine is 12.6 per million, with no known deaths. This translates to 1.26 cases of vaccine-related myocarditis per 100,000 and 0 vaccine-related deaths per 100,000.22
The data show that myocarditis appeared at a rate of 12.6 cases per million 2nd doses of any mRNA vaccine in the 21 days following vaccination.
This means if 1,000,000 people aged 12 to 15 years receive the 2nd dose, we expect 12 to 13 cases of heart inflammation.
The rate of myocarditis among big ten athletes was 2.3% of those infected with the virus.23 For an even comparison, if we have 1,000,000 teens infected, then we expect to see 23,000 cases of myocarditis.

If I’ve lost you, the critical point is that 12.6 is many magnitudes smaller than 23,000. That’s the difference.
This age bracket is older than the 12- to 15- year old group, but it is well within the under 29 years group referenced by the original author.24 In that demographic, we saw just two cases of myocarditis that required intensive care.
Put another way:
12.6/1,000,000 = 0.0000126 = 0.00126% of vaccinated people developed myocarditis.
23,000 cases of myocarditis among infected teens out of 1,000,000 infected = 2.3% of infected people developing myocarditis
The risk of myocarditis from infection in this comparison is about 1,825x greater than the risk of myocarditis from the vaccine.
The risk does seem to have a male bias, which means that boys are more likely to get myocarditis but it does not appreciably change the way we would assess the risk. Males were also more likely to die from Covid infection25 so again, this outcome in vaccines is not necessarily surprising.
As of right now, no deaths have been associated with vaccine-related heart inflammation.26
A study of adolescents hospitalized with COVID-19 found that one-third required intensive care and 5% required invasive mechanical ventilation.
Although the mortality rate for adolescents is relatively low, survivors can face persistent health problems like long COVID, which can lower their quality of life.27
7 to 20% of those under the age of 18 who catch Covid appear to be affected in ways that may be long-term, and even lifelong in some cases.28
We do not yet know of any deaths that were definitively linked to the vaccine, and we know that every single death—related or unrelated—was entered in the database and will be investigated.
There appears to be one case that is under investigation because a teen died after vaccination,29 but as discussed earlier, whether that death was a car accident, a suicide, or vaccine-related, isn’t known.
If we assume that case is related to the vaccine, which we don’t know is true, this means we have one death related to the vaccine. We should compare this to the alternative. Often we compare the risk of vaccines to the risk of nothing, which isn’t the choice we are facing.

Under 18 years, there have been 314 deaths and in the 18 to 29-year cohort, there have been 2,323 deaths.30 Another way would be to say that the risk of death is 314x higher from actual infection than from the vaccine.
I can’t tell you why people deny there have been deaths in children, but I can tell you as a 100% real person who has nothing to gain, young people have died. I tell you that as a person who knows it’s a scary time right now and that it’s hard to know who to trust. I would not give advice that I would not give to myself or my family.
Death is not the main concern for children—that’s true of many vaccine-preventable illnesses.
We do not yet know what long-term consequences the virus will bring, but we know enough that we should not be cavalier. Mayo clinic currently lists these long-term signs and symptoms as common.
Fatigue
Shortness of breath or difficulty breathing
Cough
Joint pain
Chest pain
Memory, concentration or sleep problems
Muscle pain or headache
Fast or pounding heartbeat
Loss of smell or taste
Depression or anxiety
Fever
Dizziness when you stand
Worsened symptoms after physical or mental activities
Organ-specific damage has so far included31
Heart. Imaging tests taken months after recovery from COVID-19 have shown lasting damage to the heart muscle, even in people who experienced only mild COVID-19 symptoms. This may increase the risk of heart failure or other heart complications in the future.
Lungs. The type of pneumonia often associated with COVID-19 can cause long-standing damage to the tiny air sacs (alveoli) in the lungs. The resulting scar tissue can lead to long-term breathing problems.
Brain. Even in young people, COVID-19 can cause strokes, seizures and Guillain-Barre syndrome — a condition that causes temporary paralysis. COVID-19 may also increase the risk of developing Parkinson's disease and Alzheimer's disease.
From the beginning, there was a great deal of concern because viruses like SARS and MERS had long-term effects in people who were infected. Most noteworthy were the psychological consequences.32 Some of the biggest concerns with Covid are the increased rate of mental illness diagnoses in the months after infection33 and heart complications or damage.34
Harvard recently stated that a review of 69 million people showed an increased risk for psychiatric disorders, dementia, and insomnia.35 Some speculate that low-grade inflammation in the brain may be to blame, but we can’t say for sure at this point.36 What we do know is that the virus can both infect and reproduce itself efficiently in a human brain cell.37
Will this virus cause heart failure down the road? I hope with every fiber of my being that isn’t the case and that we never find that infection causes something like shingles38 or fatal measles encephalitis39 or measles immune amnesia40 or cancer as with HPV, hepatitis viruses, and the Epstein-Barr virus,41 but we just don’t know.
We hope that none of these possibilities come to pass, but if that day should come, I want you to be the parent of a child who doesn’t face that because your child was vaccinated.

https://web.archive.org/web/20210626225755/https://alexberenson.substack.com/p/vaccines-reasons-for-concern-569
https://web.archive.org/web/20210626220801/https://www.thegatewaypundit.com/2021/06/not-making-headlines-cdc-officials-admit-hospitalizations-young-people-vaccine-actual-covid-virus-including-huge-number-heart-problems-reported/
https://web.archive.org/web/20210626230150/https://russellblakeuncensored.substack.com/p/cdc-gone-full-retard-on-vaxxing-youngsters
https://web.archive.org/web/20210625065021/https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2021-06/03-COVID-Shimabukuro-508.pdf#page=44


“Tucker Carlson Guest Falsely Claims That Israel’s Vaccine Rollout Hasn’t Worked. In Fact, the Rollout Shows That the Vaccine Works.” 2021. Accessed June 26, 2021. https://www.mediamatters.org/coronavirus-covid-19/tucker-carlson-guest-falsely-claims-israels-vaccine-rollout-hasnt-worked-fact.
https://www.theatlantic.com/ideas/archive/2021/04/pandemics-wrongest-man/618475/
Wardle, Claire. 2019. “Information Disorder: ‘The Techniques We Saw in 2016 Have Evolved.’” October 21, 2019. https://firstdraftnews.org/articles/information-disorder-the-techniques-we-saw-in-2016-have-evolved/.
https://news.mit.edu/2018/study-twitter-false-news-travels-faster-true-stories-0308
https://vaers.hhs.gov/faq.html
“Birth-18 Years Immunization Schedule.” 2021. June 16, 2021. https://www.cdc.gov/vaccines/schedules/hcp/imz/child-adolescent.html.
https://vaers.hhs.gov/faq.html
https://web.archive.org/web/20210625065021/https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2021-06/03-COVID-Shimabukuro-508.pdf#page=44
https://vaers.hhs.gov/data.html
https://web.archive.org/web/20210625065021/https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2021-06/03-COVID-Shimabukuro-508.pdf#page=44
Chu, Kevin. 1999. “An Introduction to Sensitivity, Specificity, Predictive Values and Likelihood Ratios.” Emergency Medicine Australasia: EMA 11 (3): 175–81.
https://gis.cdc.gov/grasp/COVIDNet/COVID19_5.html#virusTypeDiv
https://downloads.aap.org/AAP/PDF/AAP%20and%20CHA%20-%20Children%20and%20COVID-19%20State%20Data%20Report%206.17%20FINAL.pdf
https://services.aap.org/en/pages/2019-novel-coronavirus-covid-19-infections/children-and-covid-19-state-level-data-report/
https://www.childrensdefense.org/state-of-americas-children/soac-2021-overview/



https://jamanetwork.com/journals/jamacardiology/fullarticle/2780548
Clipping included in author’s article:

https://pubmed.ncbi.nlm.nih.gov/33063089/
https://www.npr.org/2021/06/23/1009522605/heart-inflammation-in-teens-and-young-adults-after-covid-19-vaccine-is-rare-cdc-
https://healthfeedback.org/claimreview/cdc-study-finds-five-percent-of-teens-hospitalized-due-to-covid-19-require-ventilation-vaccinating-against-covid-19-can-help-reduce-the-risk-of-severe-disease-in-teens/
https://healthfeedback.org/claimreview/cdc-study-finds-five-percent-of-teens-hospitalized-due-to-covid-19-require-ventilation-vaccinating-against-covid-19-can-help-reduce-the-risk-of-severe-disease-in-teens/
https://www.mlive.com/public-interest/2021/06/michigan-teens-death-days-after-covid-19-vaccination-being-investigated.html
https://www.statista.com/statistics/1191568/reported-deaths-from-covid-by-age-us/
https://www.mayoclinic.org/diseases-conditions/coronavirus/in-depth/coronavirus-long-term-effects/art-20490351
https://evidenceaid.org/resource/long-term-clinical-outcomes-in-survivors-of-sars-and-mers/
https://www.cidrap.umn.edu/news-perspective/2021/06/neurologic-psychiatric-conditions-common-covid-19
https://www.healthline.com/health-news/heart-damage-seen-in-50-of-people-hospitalized-with-covid-19
https://www.health.harvard.edu/blog/could-covid-19-infection-be-responsible-for-your-depressed-mood-or-anxiety-2021041922391#:~:text=A%20new%20study%20of%20electronic,disorder%2C%20dementia%2C%20or%20insomnia.
https://www.cidrap.umn.edu/news-perspective/2021/06/neurologic-psychiatric-conditions-common-covid-19
https://caat.jhsph.edu/minibrain_covid19.html
https://www.historyofvaccines.org/content/blog/chickenpox-vaccine-shingles
https://www.cdc.gov/measles/symptoms/complications.html
https://www.nature.com/articles/d41586-019-03324-7
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1994798/#:~:text=Epstein%2DBarr%20virus%2C%20human%20papilloma,that%20contribute%20to%20human%20cancers.