


Lobbyists use No True Scotsman logical fallacy to redefine abortion and then deny it can be medically necessary
The threat to life in changing the definition to suit ideology is that it doesn't change the medical definition. One should be able to hold any stance and recognize the facts in this case.
Sections
Yes, abortion can be medically necessary, despite activist claims
Changing the definition of a word is a media manipulation tactic
Miscarriage and abortion, a history
Questions without answers will cause preventable deaths, physician burnout
Yes, abortion can be medically necessary, despite activist claims
The anti-abortion activist Lila Rose has said on multiple occasions, most recently in a tweet, that removing an ectopic pregnancy is not an abortion. According to The American College of Gynecologists and Obstetricians, she’s wrong. The definition Rose implies for abortion is similarly incorrect.
Rose is not alone in making the false claim. Another incorrect but popular tweet reads, “Abortion is never medically necessary to save a woman’s life.” That’s false. The claim has popped up across social media, especially among ideologically-driven groups.


A list of outlets or fact-checking organizations with high reliability and low bias that acknowledge abortion can be necessary to save a life include:
When Rose says that treating an ectopic pregnancy does not “intentionally kill (a) child,” hence, it’s not an abortion,” the problem is that the definition of abortion is not intentionally killing a child.
It’s the loss of pregnancy before 20 weeks, according to the American Academy of Family Practice, Mayo Clinic, WHO, and the textbook Reproductive and Developmental Toxicology. Propaganda does not become reality.
Changing the definition of a word is a media manipulation tactic
Changing the definition is a manipulation tactic, described in World War-2 era texts as using “persuasive definitions.” The tactic can look like Begging the Question (petitio principii — circular reasoning) or a logical fallacy known as No True Scotsman.
No true Scotsman is a logical fallacy, meaning an error in reasoning, in which someone defends a generalization by redefining the criteria and dismissing contradictory examples.
We can explain this in simplified form:
All X are Y(It is shown that not all X are Y)All true X are YWe cannot change the definitions of words to overlook our logical inconsistencies. Inconsistencies are what is so dangerous to everyone else, but especially those who are most vulnerable, poor, and marginalized.
Miscarriage and abortion, a history
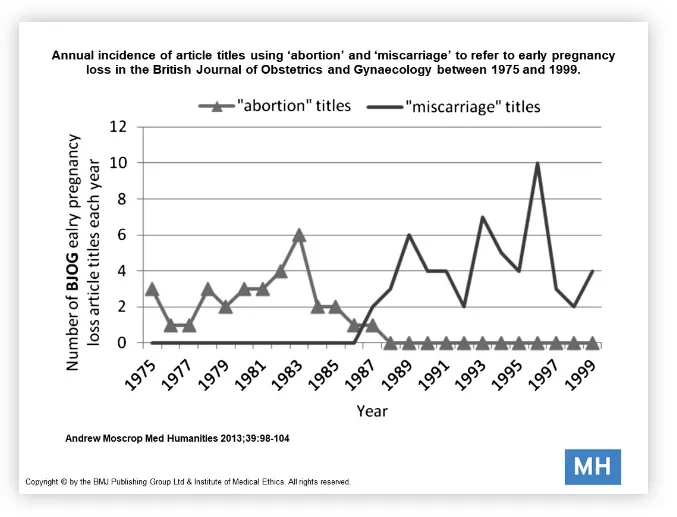
Until the 1980s, when abortion issues became partisan for the first time in US history, all pregnancy losses before 20 weeks (the exact line where it becomes a stillbirth varies a bit) were abortions.
The law does not differentiate abortion, miscarriage and premature delivery…Physicians failing to report known or suspected cases of abortion are open to suspicion of complicity and technically to criminal prosecution.—Walter W. Jetter, M.D. March 2, 1950, NEJM.
The use of the word miscarriage and its nonexistence before 1985 can be seen in the graph. The use of spontaneous abortion sharply declines and changes in a short period.

Spontaneous abortion is the loss of pregnancy naturally before twenty weeks of gestation, according to the American Academy of Family Practice, Mayo Clinic, the UK-based National Institutes for Health and Care Excellence, the WHO, the textbook Reproductive and Developmental Toxicology, and StatPearls medical definitions.
Many official sources recognize that it can also be called a miscarriage, but this does not mean lobbyists are correct in saying those aren’t abortions. The terms were and are interchangeable, even if they are not colloquially.
A 1985 letter to The Lancet shows the recency of the shift.
"It is curious that, in a language as descriptively rich as English, no clear distinction is made between a spontaneous and an induced expulsion of the contents of the uterus in early pregnancy.""Doctors use the word ‘abortion’ regardless of whether it was a spontaneous or induced event… It seems likely that the words have been interchangeable for many centuries..."
Journal articles about early pregnancy loss see a rapid shift from the use of ‘abortion,” which described all pregnancy loss, to ‘miscarriage’ as the descriptor for spontaneous ones. Miscarriage had been used interchangeably with abortion historically, perhaps for centuries.
{kind=link}
According to Professor Richard Beard, women adopted an informal meaning that gained popularity in the 1990s.
“... women’s emotional reactions to miscarriage and of the distress caused by the medical terminology of ‘spontaneous abortion’ suggests the influence of contemporaneous non-medical developments.”
“The distinction in language may also be read as part of the process of assigning meaning to those women to whom the language was applied, a process by which women who experience miscarriage could be defined as distinct from women who experience an induced abortion.”
The shift does not mean the definition changed medically or legally.
Questions without answers will cause preventable deaths, physician burnout
Logical inconsistency produces a situation where the law will be applied unequally — especially with enforcement and criminalization— and cause preventable deaths. Without answers, everyone affected by regulation will be at the mercy of the nerve of the healthcare provider or pharmacist and every healthcare provider under the fear of a zealous prosecutor.
Even before the overturn, women—mostly poor, non-white women—were charged with crimes related to pregnancy, but the addition of medical providers makes the situation more dangerous.
The oft-touted life-of-the-mother exception can and does fail. It can also lead to women being refused cancer treatment, but no legislation in the US has made the changes needed to create a workable policy. Doctors have to ask how the threat to life is calculated and who ultimately decides. The overturn means that the decision goes to someone other than the person who is pregnant in certain states. How they intend to handle the decision should be of great interest to anyone living in such a location because, without guidance, deliberation may cost your life.
How likely does death have to be for it to qualify as life-threatening?
What is the formula for calculation (no formula = guessing)? Who decides that and how?
Does the threat have to be static, or can it fluctuate? Over what period? Why?
What happens if the doctor, the state, or SCOTUS disagrees over whether the threat is extreme enough? According to major medical communities, SCOTUS has already incorporated misinformation into its opinion.
The outcomes feared by medical and legal experts are already here, and prosecution of healthcare providers will only worsen it. ACOG opposes criminalization for this reason. No one seems to recall or to have considered the “fetal assault” law in Tennesee, which had such negative consequences for the outcomes of the mother and infant, that they did away with it by choice.
At least one major anti-abortion lobbying group recommends we expand state power saying, "current realities require a much more robust enforcement regime than just reliance on criminal penalties.” They recommend “RICO-style” charges normally used for organized crime.
“What these laws do is they place physicians in an untenable position not knowing that if they serve the medical interests of their patients, they’ll be subject to criminal liability.”— Lawrence Gostin, a law professor at Georgetown University.
Arey et al. (2022) in the New England Journal of Medicine detail how constraints on physicians don’t just potentially hurt their patients.
The constraints on physicians’ autonomy to practice evidence-based medicine have created concern about the law’s long-term consequences for the medical field. SB8 has taken a toll on clinicians’ mental health; some physicians report feeling like “worse doctors,” and some are leaving the state. As a result, clinicians worry that pregnant Texans are being left without options for care and without doctors capable of providing it.
The brief of Amici Curiae from the American College of Obstetricians and Gynecologists, American Medical Association, American Academy of Family Physicians, American Academy of Nursing, American Academy of Pediatrics, American Association of Public Health Physicians, and others stated the problem succinctly:
Indeed, the Ban reflects a fundamental misunderstanding and misrepresentation of the science of fetal development.
Snippets from the amicus brief from nearly all of the respected, relevant medical institutions warn about the threats the overturn poses:
The Ban also impermissibly intrudes into the patient-physician relationship by limiting a physician's ability to provide the health care that the patient, in consultation with her physician, decides is best for her health. Moreover, the Ban undermines long-standing principles of medical ethics and places clinicians in the untenable position of choosing between providing care consistent with their best medical judgment, scientific evidence, and the clinicians' ethical obligations or risk losing their medical licenses. The provision of safe abortion services after careful consultation with a patient does not demean the practice of medicine. But infringement on a clinician's ability to honor patient autonomy by allowing patients to make their own health care decisions, certainly does.
They continue:
It is untenable to force a pregnant patient to wait until her medical condition escalates to the point that "an abortion is necessary to preserve [her] life" or her pregnancy creates a "serious risk of substantial and irreversible impairment of a major bodily function" before being able to seek potentially life-saving care. Miss. Code § 41-41-191. Nor should physicians be put in the impossible position of either letting a patient deteriorate until one of these conditions is met or face possible loss of their medical licenses for performing an abortion in contravention of the Ban. In forcing physicians to wait until a patient is close enough to death that they will risk their license to practice medicine to save her life by providing needed abortion care, the State indefensibly jeopardizes patients' health.
Reuters has high-quality reporting except on topics related to Russia.
Tweet this please. Spread the word